
The race to biomarkers — but are we measuring the right ones?
More is not always better. A look at what the at-home testing market is actually selling, what it's missing, and what a rational panel should look like.
This is the third piece in the Late Night Convo series. The first was about how we rebuilt Biostarks as an AI-native company. The second read the M&A wave reshaping the category. This one is about something that has been bothering me for a while: the industry's obsession with biomarker count, and what that obsession is causing us to miss.
The number race
The at-home biomarker testing market has developed a peculiar competitive logic: more markers equals better product. Function Health markets 100+ biomarkers. Ultrahuman tests roughly 100 twice a year. Newer entrants push higher. The marketing practically writes itself — each launch announces a new ceiling, each competitor scrambles to match it.
This is understandable. Biomarker count is legible to consumers in a way that panel design is not. Saying "we test 150 biomarkers" lands. Saying "we test the right 60" requires explanation.
The logic gets stranger at the edges. Some genomic testing companies — 23andMe's successors, various longevity platforms — now market themselves as measuring "500+ biomarkers." The number is not technically false, but it is misleading in a way that matters. What they are reporting is not biomarker status. It is genetic variants: specific sequences in your DNA that correlate statistically with a likelihood of having a particular biomarker profile. That is interesting science. It is not the same as measuring your Vitamin D level on a given day.
The distinction is not subtle. A genomic test can tell you that you carry a variant associated with lower Vitamin D conversion efficiency. It cannot tell you that your serum 25(OH)D is at 22 ng/mL right now, that this is insufficient, and that you need to address it. For that, you need blood.
Inflating genomic reports with biomarker language inflates the count and muddies the category. It is worth naming clearly.
What more markers actually buys you
Setting aside the genomics conflation, there is still a real question about whether more lab markers produces better health insight. The honest answer is: it depends entirely on which markers you add.
Function Health's Labcorp-based panels, Ultrahuman's quarterly labs, Superpower's Quest-routed offering — they all sit inside the same operating logic. The one I'll walk through is Oura Labs, for the straightforward reason that I have an actual result report to work from rather than only the marketing page. Sixty-five-plus biomarkers. Phlebotomy draw. Fifteen vials of blood. Oura has put real effort into the experience layer — the interface is clean, the results well-presented.
When imported into Biostarks Open Labs, panels like this one read less like a preventive health product and more like the immunology and hematology workup my father received during his six weeks in hospital after a ski accident. Useful in that context. Not what most people booking a wellness panel have in mind.
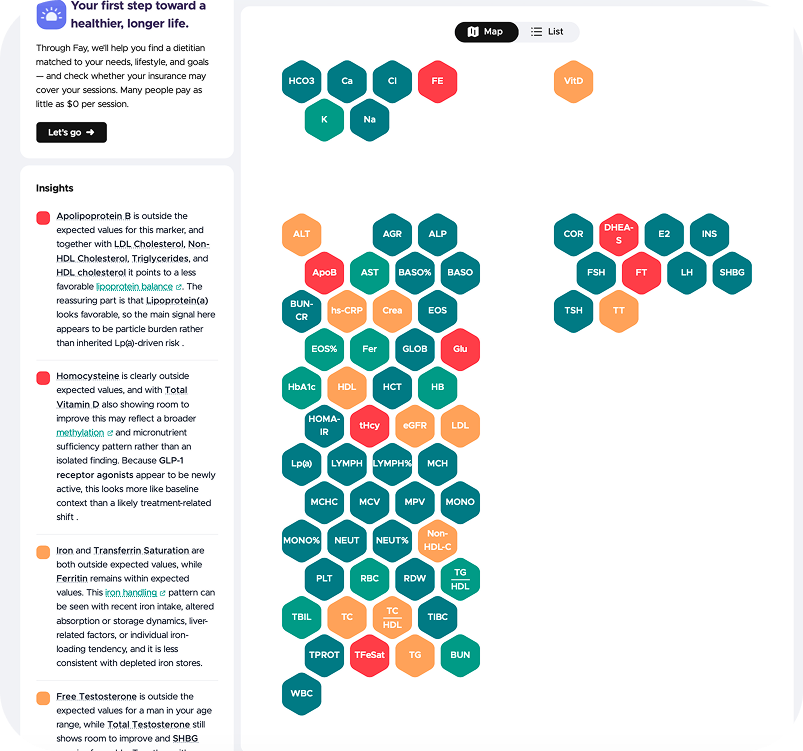
When you map the 65 markers by domain, more than half — 37 of them — fall into clinical monitoring: a complete blood count with full leukocyte differential (twenty markers alone), eight liver function markers, four electrolytes, kidney markers, and iron transport indices. This is the infrastructure of hospital diagnostics. It is the right test when a physician needs to rule out infection, anaemia, hepatocellular damage, or electrolyte crisis.
For a healthy adult optimising their health, most of those markers will be normal, will convey no actionable signal, and will contribute nothing to a protocol change. They add up to a medically thorough result, but not a preventively useful one.
The metabolic section is genuinely strong: glucose, HbA1c, fasting insulin, and HOMA-IR together constitute a proper glycaemic picture that most standard panels do not include. The lipid section goes beyond the conventional — ApoB and Lp(a) alongside the standard lipid fractions is modern, appropriate cardiometabolic coverage. The sex hormone panel is complete: total and free testosterone, SHBG, DHEA-S, estradiol, FSH, LH.
These are the panel's highlights, and they are real. But then consider what fifteen vials of blood did not buy.
One vitamin. Vitamin D, and nothing else. No B12. No folate — despite homocysteine being measured, which makes the absence of its upstream drivers (B12, folate, B6) particularly strange. No Vitamin A, E, K, or C.
Zero minerals. Magnesium — arguably the most commonly deficient micronutrient in a population under chronic stress — is absent. No zinc, no selenium, no copper.
No fatty acid profile. No omega-3 index, no EPA/DHA, no arachidonic acid ratio. No amino acid panel.
Nothing in the longevity or oxidative stress space. No NAD+ precursors, no 8-OHdG, no GDF-15, no biological age markers, no environmental load markers such as heavy metals or microplastic-associated signals.
The result is a panel that is excellent at detecting the kinds of things a clinician looks for in a sick patient — and limited in its ability to guide the kinds of interventions a well person could actually act on tomorrow. As Jen Gunter, MD, put it in a Nature feature on the DTC testing industry: "We all mistake data for knowledge." [^6]
Why does this happen? This is not an Oura-specific design choice — it is the category's default. The at-home testing market largely runs on incumbent lab infrastructure — pipelines originally built to support hospital diagnostics and urgent care. That infrastructure is excellent at what it was designed for. But it carries a design bias: it optimises for clinical completeness over preventive actionability.
The pattern shows up directly in this panel. The full CBC differential — twenty markers covering neutrophils, lymphocytes, monocytes, eosinophils, basophils — is hospital-grade infection and anaemia screening; in a well adult, it will almost always be normal and actionable on nothing. The electrolyte panel (sodium, potassium, chloride, bicarbonate) is ICU monitoring — stable in any healthy person not in acute distress. The eight liver function markers are diagnostic tools for hepatocellular or cholestatic disease, not levers for health optimisation.
A hospital panel dressed as preventive health.
The problem is not with Oura, or with any individual brand. Function, Superpower, Ultrahuman, and the broader cohort of premium at-home players are all following the industry's dominant logic: route through existing lab networks, maximise marker count, present beautifully. The problem is with the logic itself. Oura is simply the case where I happen to have the numbers to show it.
What a rational panel architecture looks like
If the goal is actionability — not diagnostic completeness — the design problem is different. You are not building a panel to catch what is wrong. You are building a panel to tell a person what to change.
That reframe suggests a layered architecture — one that maps, interestingly, onto the taxonomy a January 2026 narrative review in Diagnostics independently drew: well-validated markers with clear actionable pathways, markers with disease associations but limited intervention options, and early-stage markers with promising signals but insufficient population-level validation.[^2] The clinical literature is arriving at the same hierarchy from a different direction.
Layer one: nutritional status. Vitamins, minerals, fatty acids, amino acids. This is where most intervention potential sits for the average health-conscious person — and the epidemiology makes the case more forcefully than any product argument could.
A 2023 Harvard and UC Santa Barbara modelling study published in The Lancet Global Health, covering 185 countries, found that more than 5 billion people do not consume enough iodine, vitamin E, or calcium, and more than 4 billion fall short on iron, riboflavin, folate, and vitamin C.[^3] In the United States specifically, NHANES data show that 94% of the population does not meet the daily requirement for vitamin D, 88% for vitamin E, and 52% for magnesium.[^4]
The point is not that everyone is deficient in the same things. It is the opposite: almost everyone has at least one micronutrient gap, but each person's gap is different. Mark Hyman has described this as "long-latency deficiency disease" — chronic insufficiencies that drive cardiovascular risk, cognitive decline, and metabolic dysfunction over decades, entirely below the threshold that clinical medicine, built around acute deficiency, is designed to catch.[^1] A blanket recommendation to take vitamin D helps no one optimise. Measuring where you specifically fall short — and acting on it — is what makes the nutritional layer worth starting with. The feedback loop is tight: supplement this, adjust that diet, retest in twelve weeks. No other layer of health testing offers that cadence.
Layer two: metabolic health. This layer extends and contextualises the nutritional foundation — it does not replace it. The full set of nutritional markers from Layer 1 remains relevant here; what is added is glycaemic control, lipid balance, deeper inflammation markers, liver and kidney function, and the hormonal axes that govern metabolic regulation. This is where chronic disease risk accumulates over years. The interventions are slower — dietary pattern shifts, body composition changes, sometimes clinical referral — and the longitudinal picture matters more than any single result. It belongs in layer two of a health journey because the nutritional baseline has to be established first: you cannot reliably interpret a rising homocysteine or worsening insulin sensitivity without knowing the B-vitamin and magnesium status that may be driving it.
Layer three: environmental health and frontier longevity. This layer has several distinct faces that are worth keeping separate.
The environmental health side — microplastics, heavy metals, mould metabolites, PFAS, persistent organic pollutants — is increasingly measurable and increasingly relevant. Exposure burden is real, population prevalence is underappreciated, and the intervention logic (reduce source, support detoxification pathways) is reasonably clear. This is frontier in terms of mainstream adoption, not in terms of scientific validity.
Oxidative stress sits just below that on the readiness curve. Markers like 8-OHdG — the most direct measure of oxidative DNA damage available in blood — and 8-iso-PGF2a, an isoprostane that reflects lipid peroxidation independent of inflammation, give a concrete signal of cellular oxidative load. The antioxidant defense side is equally important: GSH(total glutathione) and GPX (glutathione peroxidase) together describe how well the body neutralises free radicals, while CoQ10 captures mitochondrial antioxidant capacity specifically. The FORT/FORD ratio — oxidative load against antioxidant defense — compresses this into a single actionable picture. These markers have validated reference ranges and reasonably clear intervention pathways (dietary, supplementation, lifestyle). They are not as mature as Layer 2, but they are close.
Gut health is the third sub-layer, and arguably the most underappreciated in consumer testing today. TMAO(trimethylamine N-oxide) connects gut microbiome composition to cardiovascular risk — elevated TMAO is one of the better-validated gut-derived biomarkers for atherosclerosis progression. DAO (diamine oxidase) reflects intestinal barrier integrity and histamine metabolism, a combination that matters far beyond allergy. Zonulin is the most direct available proxy for intestinal permeability — the leaky gut signal most panels ignore entirely. Within gut health, IDO activity deserves special attention. IDO (indoleamine 2,3-dioxygenase) is the enzyme that diverts tryptophan away from serotonin synthesis and toward the kynurenine pathway when the immune system is chronically activated. The KYN/TRP ratio is its activity proxy — elevated in chronic inflammation, depression, and accelerated ageing. The pathway then branches: toward kynurenic acid (neuroprotective) or quinolinic acid (neurotoxic), and the QUIN/KynA ratio captures which direction it is heading. IPA (indole-3-propionic acid) and the IPA/TRP ratio represent the alternative, gut-bacteria-dependent tryptophan route — anti-inflammatory, neuroprotective, and increasingly recognised as a longevity-relevant metabolite. Taken together, the kynurenine pathway markers give a mechanistic view of the gut-brain-immune axis that no standard panel touches.
The frontier longevity side proper is more genuinely unsettled — and worth being honest about. Most commercial biological age scores are built on proxies derived from routine bloodwork: red blood cell indices, albumin, creatinine, glucose, standard lipid fractions. These measure downstream consequences of ageing rather than its underlying pace. The more interesting candidates are mechanistic. IL-6 and TNF-α — pro-inflammatory cytokines whose chronic low-grade elevation, inflammaging, is one of the most consistent predictors of accelerated multi-organ decline. GDF-15, a stress-response cytokine released by damaged mitochondria, is emerging as one of the strongest single-marker predictors of biological age and all-cause mortality across large cohort studies. BDNF (Brain-Derived Neurotrophic Factor) tracks neuroplasticity and cognitive resilience; its decline precedes measurable cognitive deterioration by years. Humanin, a mitochondria-derived peptide, correlates inversely with insulin resistance, cardiovascular risk, and cognitive impairment — one of the few markers that speaks directly to mitochondrial signalling rather than its metabolic effects.
None of these are ready for a first-panel context. Reference ranges are still population-calibrating, and translating a single result into a protocol requires interpretive infrastructure most platforms have not built. But they represent the direction the field is moving — away from ageing-as-metabolic-proxy and toward ageing-as-biological-process.
There is also a biological argument for keeping this entire layer last in the sequence: biochemist Bruce Ames' Triage Theory holds that when micronutrients are scarce, the body rations them toward short-term survival at the expense of long-term DNA repair and cellular maintenance.[^5] You cannot meaningfully interpret inflammaging markers or IDO pathway activity in a person whose magnesium, omega-3, or folate status is unknown — because the deficiencies may be driving the signal.
The industry's current tendency is to conflate these layers, or to skip layer one in favour of the clinical credibility of layer two. The result is panels that look serious but leave the most motivated users without the information most likely to change their behaviour.
How this shapes what we are building
At Biostarks, this layered logic maps directly onto our product architecture, which is worth making explicit.
The differentiation starts with the analytical platform before it reaches the panel design. Most at-home testing — and most standard lab infrastructure that consumer brands route through — runs on immunoassay: a technology well-suited to hormones, a handful of proteins, and standard clinical chemistry markers. It is the backbone of Quest, Unilabs, and the broader hospital lab network, which is precisely why panels built on it end up looking like clinical panels. Immunoassay cannot measure amino acids, fatty acids, most vitamins in their active forms, methylation metabolites, or the IDO pathway markers discussed above. The analyte categories are simply outside its reach.
Biostarks runs on mass spectrometry — high-resolution LC-MS/MS for metabolites, fatty acids, amino acids, and vitamins; ICP-MS for minerals. This is not just what makes the dry blood spot model work at home. It is what unlocks the nutritional layer in the first place. The depth of analyte coverage is not a panel design choice layered on top of standard infrastructure — it is a consequence of building on a different analytical foundation entirely.
Our Tier 1 is the Nutrition Panel. Thirty biomarkers covering vitamins, minerals, fatty acids, amino acids, and iron metabolism — everything that is directly actionable and has a short protocol-to-result feedback cycle. Four drops of blood, finger-prick, no phlebotomy. This is where we think the consumer health conversation should start, and where most of the category is currently underserving people.
Tier 2 is the Metabolic Health Panel. It is designed explicitly as an extension of the Nutrition Panel: it includes all the nutritional markers of Tier 1 and expands on them with lipid profiles, glycaemic markers, inflammatory signals, hormonal axes, and metabolic depth. Thirty-nine biomarkers in the current panel, growing toward ninety-one in the target roadmap. The nutritional foundation is not replaced at this tier — it is contextualised. Elevated homocysteine reads differently when you also know the B12, folate, and betaine status. An insulin resistance signal is harder to act on without the magnesium and omega-3 picture alongside it.
The Longevity NAD+ panel is currently offered as a standalone — measuring intracellular NAD+ alongside its key cofactors (magnesium, zinc, selenium). The intention is for it to evolve into a modular add-on to Tiers 1 and 2, not a starting point. Longevity markers interpreted without a nutritional and metabolic foundation underneath them are hard to act on. Interpreted with it, the picture becomes coherent.

The sequencing matters as much as the content. Knowing your homocysteine is elevated is only useful if you also know your B12 and folate status and understand what to do with the combination. Most panels give you the former and skip the latter. We think that is the wrong trade-off.
What do you do with all of this?
Panel design is one question. The one that follows is harder: once you have forty, seventy, a hundred biomarkers longitudinally for a person, what do you actually hand them?
The category's default answer is a biological age. One number, lower-is-better, the emotional centre of most consumer longevity products. The marketing logic is clean — everyone understands the shape of an age — but the science underneath it is thinner than the interface suggests.
Most biological age scores in production today trace back to Levine's Phenotypic Age, published in 2018, which was trained on NHANES clinical chemistry data: albumin, creatinine, glucose, CRP, red blood cell distribution width, alkaline phosphatase, white blood cell count, lymphocyte percentage, mean corpuscular volume — plus chronological age.[^7] It is a carefully validated paper. But look at the input list. It is, almost line for line, the hematology-and-basic-metabolic panel that hospital labs have been running for decades. PhenoAge worked because those were the markers available in large epidemiological datasets, not because they represent the best mechanistic understanding of how a person is ageing.
So the irony compounds. The industry is sold on biological age as the synthetic output of a comprehensive panel — and the most widely deployed version of that output is built on exactly the clinical-panel infrastructure that the earlier part of this piece argued is the wrong starting point for preventive health. You end up summarising a panel mostly designed to detect disease into a single number mostly trained on the markers detecting that disease. It is internally consistent. It is not the same as telling someone how well they are ageing.
More mechanistic alternatives exist — GrimAge and DunedinPACE, built on DNA methylation; emerging work around GDF-15, IL-6, and the mitochondrial-signalling peptides referenced in Layer 3 above. Methylation clocks require sequencing rather than standard blood; the cytokine work is not yet validated at the population scale needed to anchor a consumer product. The field is moving, but the most common score the consumer actually sees on their dashboard today is still a linear combination of clinical chemistry markers their grandparents would have recognised.
We are exploring a different framing at Biostarks, and it is worth being upfront that this is under active exploration rather than something we are selling today. Rather than collapse a person's biomarker profile into a single age number, we are looking at biological age as a distance measurement — how far a person's multi-dimensional biomarker profile sits from the centroid of what a healthy reference population looks like, and in which directions that distance is driven.
The output of that framing is not "you are 42 biologically" but something closer to "your nutritional layer sits at the 75th percentile of healthy 40–49 year olds, your metabolic layer at the 30th, your oxidative stress load places you in the upper quartile for your age cohort." A stratified risk view rather than a single score. The upside is that it maps directly to intervention — each dimension has a clear lever. The downside is that it is harder to put on a marketing page. "Your biological age is 39" sells rings and subscriptions. "You are three standard deviations off the healthy-population mean on oxidative load" does not.
We are still calibrating this. The reference population work is harder than the clock work — you need to be honest about what "healthy" means, about age-cohort stratification, about sex and ethnicity effects. But the direction feels right: if the panel is supposed to tell a person what to change, the summary of the panel should do the same thing at a higher level of abstraction.
The real competitive question
The market's current competition is mostly about who can measure more. That competition will eventually converge on a ceiling — there are only so many validated blood biomarkers — and when it does, the question will shift to which company built the most coherent framework around them.
More markers will not differentiate anyone in the long run. The differentiation will come from panel design logic, interpretive depth, and the quality of the protocol that follows. Getting to 100 biomarkers is a milestone. Building a product where the 100th biomarker is there because it belongs — because it completes a picture that was already useful — is the harder thing, and the more durable one.
We are early. The category is still mostly competing on volume. But the conversation is starting to shift, and I expect the next cycle of product evolution to be less about what is measured and more about why — and less about collapsing a panel into a single number, more about telling a person, with specificity, which direction to move.
More soon.
— Romain Dorange, CEO & Co-Founder, Biostarks
This is the third piece in the Late Night Convo series on building an AI-native at-home biomarker testing company.
References
[^1]: Hyman, M. (2013). Setting the record straight on supplements and long-latency deficiency disease. drhyman.com. https://drhyman.com/blog/2013/11/18/setting-record-straight-supplements/
[^2]: Wiedermann, C.J. et al. (2026). Predictive Biomarkers for Asymptomatic Adults: Opportunities, Risks, and Guidance for General Practice. Diagnostics, 16(2), 196. https://doi.org/10.3390/diagnostics16020196
[^3]: Passarelli, S. et al. (2024). Global estimation of dietary micronutrient inadequacies: a modelling analysis. The Lancet Global Health, 12(10). https://doi.org/10.1016/S2214-109X(24)00276-6
[^4]: Wallace, T.C. et al. (2020). Dietary supplement use in the United States, 2011–2012. Nutrients, 12(7). Data sourced from NHANES 2003–2016 via the Linus Pauling Institute Micronutrient Information Center. https://lpi.oregonstate.edu/mic/micronutrient-inadequacies/overview
[^5]: Ames, B.N. (2018). Prolonging healthy aging: Longevity vitamins and proteins. PNAS, 115(43), 10836–10844. https://doi.org/10.1073/pnas.1809045115
[^6]: Willyard, C. (2025). Home medical tests miss the mark. Nature, 633. https://doi.org/10.1038/d41586-025-02106-8
[^7]: Liu, Z., Kuo, P.L., Horvath, S., Crimmins, E., Ferrucci, L., & Levine, M. (2018). A new aging measure captures morbidity and mortality risk across diverse subpopulations from NHANES IV: A cohort study. PLOS Medicine, 15(12), e1002718. https://doi.org/10.1371/journal.pmed.1002718